Thyroid Cancer Treatment in Delhi NCR
The thyroid is a small, butterfly-shaped gland sitting at the front of your neck, just below the Adam’s apple. It produces hormones, mainly T3 and T4, that regulate your metabolism, heart rate, body temperature, and energy levels. When cells in this gland mutate and begin growing uncontrollably, it results in thyroid cancer.
Thyroid cancer is the most common endocrine malignancy in the world, and its incidence has been rising in India over the past two decades. In Delhi NCR alone, a significant number of new cases are diagnosed every year, many of them in younger patients, including women between the ages of 25 and 50.
The good news is that thyroid cancer, particularly when caught early, is among the most treatable cancers. With the right surgical team and a proper treatment plan, the majority of patients recover fully and go on to live normal, active lives.
Types of Thyroid Cancer
Thyroid cancer is not a single disease. The type you have determines how aggressive it is, how it is treated, and what your long-term prognosis looks like.
- Papillary Thyroid Carcinoma (PTC) accounts for roughly 80–85% of all thyroid cancer cases. It grows slowly, usually stays within the thyroid or spreads only to nearby lymph nodes, and responds well to surgery and radioactive iodine. Even in cases with lymph node involvement, outcomes are excellent with proper treatment.
- Follicular Thyroid Carcinoma makes up around 10–15% of cases. Unlike papillary cancer, it tends to spread via the bloodstream to distant organs like the lungs or bones rather than through lymph nodes. It is still considered a well-differentiated cancer and is generally very treatable.
- Medullary Thyroid Carcinoma (MTC) originates in the parafollicular C-cells, which produce calcitonin rather than thyroid hormone. About 25% of medullary cases are hereditary, linked to mutations in the RET gene. This type does not respond to radioactive iodine, making complete surgical removal especially critical.
- Anaplastic Thyroid Carcinoma is rare, accounting for less than 2% of cases, but highly aggressive. It grows rapidly and is often diagnosed at an advanced stage. This type requires immediate, high-level specialist care and a multidisciplinary treatment approach.
- Thyroid Lymphoma is uncommon and arises from immune cells within the thyroid. It is typically treated with chemotherapy and radiation rather than surgery.
Symptoms of Thyroid Cancer
One of the challenges with thyroid cancer is that it often produces no symptoms in the early stages. Many cases are discovered incidentally, during a neck ultrasound done for another reason, or when a patient or doctor notices a swelling in the neck.
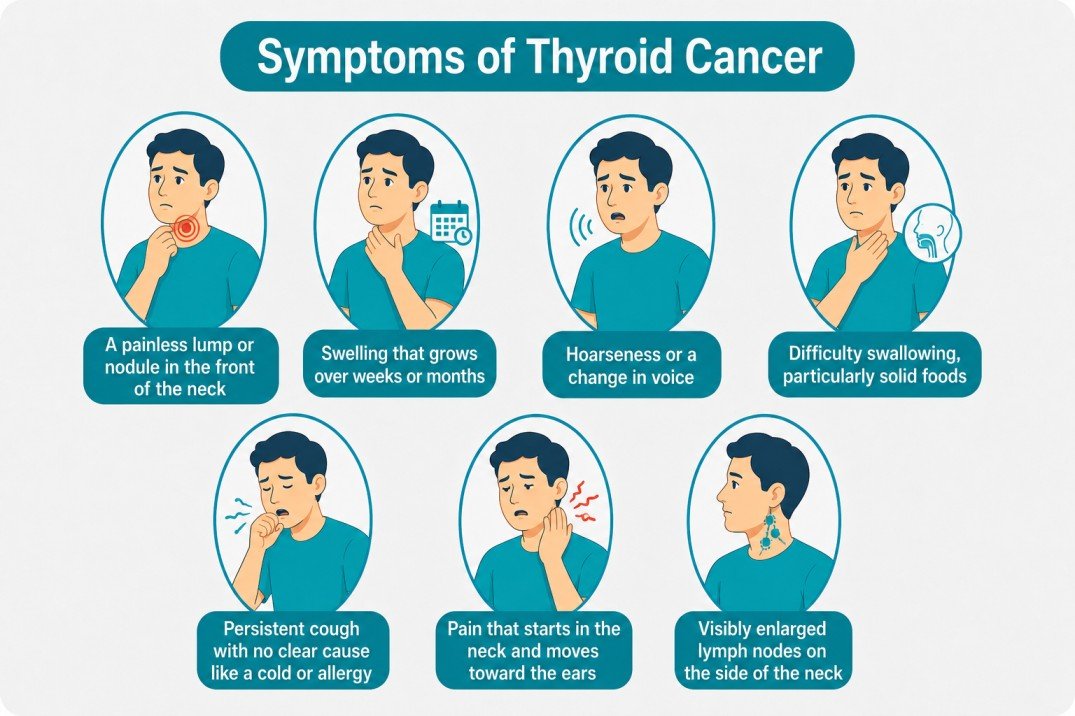
When symptoms do appear, they typically include:
- A painless lump or nodule in the front of the neck
- Swelling that grows over weeks or months
- Hoarseness or a change in voice that persists beyond two to three weeks
- Difficulty swallowing, particularly solid foods
- Persistent cough with no clear cause like a cold or allergy
- Pain that starts in the neck and moves toward the ears
- Visibly enlarged lymph nodes on the side of the neck
A neck lump does not automatically mean cancer. The large majority of thyroid nodules are benign. But any persistent swelling in the neck should be evaluated by a specialist. Early detection makes a significant difference in how straightforward treatment can be.
Reach Out for Expert Care
How Is Thyroid Cancer Diagnosed?
A thorough diagnosis involves several steps, each building a clearer picture of whether cancer is present, what type it is, and how far it has spread.
- Neck Ultrasound is usually the first investigation. It shows the size, shape, and character of any thyroid nodule, whether it has irregular borders, internal calcifications, or abnormal blood flow, all of which can indicate a higher risk of malignancy.
- Fine Needle Aspiration Cytology (FNAC) is the standard next step for any suspicious nodule. A thin needle draws cells from the nodule for microscopic examination. The procedure takes a few minutes, requires no anaesthesia, and accurately identifies most thyroid cancers.
- Blood Tests include thyroid function tests (TSH, T3, T4), thyroglobulin levels (a tumour marker for papillary and follicular cancers), and calcitonin levels (elevated in medullary thyroid cancer). These also serve as a baseline for post-treatment monitoring.
- CT Scan or MRI of the neck and chest is recommended when the cancer appears to have spread beyond the thyroid, to lymph nodes, the windpipe, or distant organs. This helps with surgical planning and staging.
- Genetic Testing is advised when medullary thyroid cancer is suspected or confirmed, to check for RET mutations. Family members may also need screening in such cases.
Stages of Thyroid Cancer
Thyroid cancer is staged from I to IV based on tumour size, lymph node involvement, and whether distant spread has occurred. For papillary and follicular cancers, age at diagnosis also plays a role, patients under 55 are staged differently.
Stage I – The cancer is confined to the thyroid. For patients under 55 with papillary or follicular cancer, Stage I includes cases where lymph nodes are involved but no distant spread has occurred. Prognosis is excellent and surgery alone is often curative.
Stage II – For patients under 55, Stage II means the cancer has spread to distant organs like the lungs or bones. For patients over 55, it refers to a tumour larger than 4 cm still within the thyroid, or with minor spread to surrounding tissue. Treatment is still highly effective.
Stage III – The cancer has grown into nearby neck structures such as the windpipe, larynx, or esophagus, or has spread significantly to regional lymph nodes. Surgery remains the primary treatment, typically followed by radioactive iodine and hormone suppression therapy.
Stage IV – The cancer has spread extensively into surrounding structures or to distant organs. Stage IVA and IVB refer to local invasion; Stage IVC involves distant metastasis. A combination of surgery, targeted therapy, and in some cases clinical trials is used. Even at this stage, many patients with papillary or follicular cancer can be managed effectively.
Treatment Options for Thyroid Cancer
Surgery
Surgery is the first-line treatment for almost all types of thyroid cancer. The extent depends on the type, size, and stage.
- Lobectomy removes only the affected lobe of the thyroid and is considered for small, low-risk papillary cancers confined to one side.
- Total Thyroidectomy removes the entire thyroid gland. This is the standard approach for most thyroid cancer cases and allows for accurate staging, complete tumour removal, and effective use of radioactive iodine therapy afterward.
- Neck Dissection is performed when cancer has spread to lymph nodes in the neck. The affected nodes are removed while carefully protecting the parathyroid glands and the recurrent laryngeal nerve, which controls the voice.
The skill and experience of the surgeon directly affects outcomes. These structures leave very little margin for error.
Robotic Thyroidectomy: Surgery Without a Neck Scar
For suitable patients, robotic thyroidectomy offers complete, precise thyroid cancer surgery with no visible incision on the neck.
Instead of a traditional cut across the front of the neck, the procedure is performed through small incisions in the armpit or behind the ear. A robotic surgical system, guided entirely by the surgeon, delivers magnified, three-dimensional visualisation and finely controlled instrument movement deep inside the neck.
Dr. Surender Kumar Dabas, one of the best robotic cancer surgeons in India, performs robotic thyroidectomy at Manipal Comprehensive Cancer Centre, Delhi NCR. With over 5,000 robotic procedures performed and the highest number of robotic head and neck surgeries in Asia, Dr. Dabas brings a level of experience in this technique that very few surgical oncologists in Delhi can match.
Clinical outcomes of robotic thyroidectomy, in experienced hands, are comparable to open surgery for cancer control, with the added benefits of less postoperative pain, faster recovery, and no scar on the neck. For younger patients and professionals particularly conscious of cosmetic outcomes, this difference is meaningful.
A full breakdown of the procedure, patient selection criteria, and what to expect is available on the dedicated Robotic Thyroidectomy page.
Radioactive Iodine (RAI) Therapy
After total thyroidectomy for papillary or follicular thyroid cancer, most patients receive radioactive iodine therapy. Because thyroid cells are the only cells in the body that absorb iodine, a radioactive form can destroy any remaining thyroid tissue or spread cells, including those in lymph nodes or distant sites.
The treatment is taken orally as a capsule or liquid. Patients follow a low-iodine diet for two weeks beforehand and may temporarily stop thyroid hormone medication to raise TSH levels, which improves iodine uptake. A short period of isolation is required afterward to limit radiation exposure to others.
Thyroid Hormone Suppression Therapy
Once the thyroid is removed, patients take a daily synthetic thyroid hormone tablet (levothyroxine) for life. For many thyroid cancer patients, the dose is intentionally kept slightly higher than a standard replacement dose. This suppresses TSH, which would otherwise act as a growth signal for any residual thyroid cancer cells. The suppression level is gradually reduced over time based on the patient’s risk category and response to treatment.
External Beam Radiation Therapy
External radiation is not routine for most thyroid cancers. It is used in selected cases, primarily anaplastic thyroid cancer, or when surgery cannot fully remove the tumour and radioactive iodine is ineffective. It may also help control symptoms in advanced disease.
Targeted Therapy and Immunotherapy
For advanced, recurrent, or radioactive iodine-resistant thyroid cancers, targeted drugs block the specific molecular pathways driving cancer cell growth. Lenvatinib and sorafenib are approved for differentiated thyroid cancers. Vandetanib and cabozantinib are used for medullary thyroid cancer. Immunotherapy combinations are being studied in clinical trials for anaplastic thyroid cancer with emerging positive results in select patients.
Cost of Thyroid Cancer Surgery in Delhi NCR
Thyroid cancer surgery cost in Delhi NCR varies depending on the type of procedure, open thyroidectomy or robotic thyroidectomy, the hospital, and the extent of the disease. To get an accurate estimate based on your diagnosis and treatment plan, you can contact Dr. Surender Dabas’s team directly for a consultation.
Life After Thyroid Cancer Treatment
Most thyroid cancer patients do not need to alter their lifestyle significantly after treatment. Follow-up care typically includes:
- Neck ultrasound every 6-12 months in the first few years
- Thyroglobulin blood test to detect any recurrence
- Whole body scan with radioactive iodine if recurrence is suspected
- Ongoing levothyroxine medication with periodic dose adjustments
Recurrence in well-differentiated thyroid cancer is uncommon when initial treatment is thorough. When it does occur, it is often in lymph nodes and can usually be treated effectively with repeat surgery or RAI.
Why Does Surgeon Experience Matters in Thyroid Cancer?
Thyroid surgery has very little margin for error. The recurrent laryngeal nerve, which controls your voice, runs directly behind the thyroid. The four parathyroid glands, critical for calcium regulation, sit tucked against the thyroid capsule. An injury to either can cause permanent voice changes or calcium deficiency.
Choosing a best surgical oncologist in Delhi who performs a high volume of thyroid surgeries, particularly one who has made robotic cancer surgery a core part of their practice, significantly reduces this risk.
Dr. Surender Kumar Dabas at Manipal Comprehensive Cancer Centre has performed over 30,000 cancer surgeries. He has trained surgeons at institutions including AIIMS, TMH Mumbai, and Apollo Hospitals. Patients from Gurgaon, Rohtak, Meerut, Muzaffarnagar, and across North India consult him for complex thyroid cancer cases, second opinions, and robotic thyroidectomy in Delhi NCR. If you are looking for the best robotic surgeon in Delhi for thyroid cancer, Dr. Dabas is among the most experienced names in the country.
Conclusion
Thyroid cancer, for all the anxiety a diagnosis brings, is one of the few cancers where the odds are genuinely in the patient’s favour. With the right diagnosis, the right surgeon, and a structured follow-up plan, most people who walk into a consultation room with a thyroid cancer diagnosis walk out the other side of treatment with their lives largely intact. What makes the difference is not just the treatment protocol, it is who performs it and how. Whether you are considering a standard thyroidectomy or exploring robotic thyroidectomy in Delhi NCR as a scarless alternative, the priority is finding a surgical oncologist in Delhi with the volume, the precision, and the specific expertise in thyroid cancer surgery that this procedure demands. Dr. Surender Kumar Dabas, widely regarded as one of the best robotic cancer surgeons in India, brings all of that to every case, from straightforward papillary cancers to complex, multi-nodal disease. If you have been diagnosed, or are waiting on results, do not delay getting a specialist opinion. Early action is still the single biggest factor in a good outcome.

Dr. Surender Dabas' Medical Content Team
Dr. Surender Dabas' Medical Content Team is committed to providing accurate, reliable, and easy-to-understand information on cancer care. Working closely with oncology experts, the team ensures that every article is medically reviewed, up-to-date, and designed to help patients and their families better understand cancer, treatment options, and recovery.
