Pancreatic Cancer Treatment in Delhi NCR
The pancreas is a gland about 15 centimetres long, tucked behind the stomach in the upper abdomen. It does two important jobs: it produces digestive enzymes that break down food, and it makes hormones, including insulin and glucagon, that regulate blood sugar. When cancer develops in the tissues of the pancreas, it disrupts both functions and, left untreated, spreads quickly to surrounding organs and blood vessels.
Pancreatic cancer is one of the more serious cancer diagnoses a patient can receive, not because it is untreatable, but because it is rarely caught early. The pancreas sits deep in the abdomen, far from the body’s surface, and early tumours typically cause no symptoms. By the time most patients feel something is wrong, the cancer has often already grown or spread.
This is why awareness of risk factors and early specialist evaluation matters so much. When pancreatic cancer is caught at a localised stage, before it has spread, surgery offers a genuine chance of cure. And with advances in robotic surgery, those operations are now safer and more precise than they have ever been.
Patients from Rohtak, Kanpur, Delhi, Gurgaon, and across North India consult Dr. Surender Kumar Dabas, one of the best pancreatic cancer doctors in India, for surgical evaluation and treatment at Manipal Comprehensive Cancer Centre, Delhi NCR.
Understanding the Pancreas
The pancreas has two functional components. The exocrine pancreas produces digestive enzymes that travel through a network of ducts into the small intestine. The endocrine pancreas consists of clusters of cells called the islets of Langerhans, which produce insulin, glucagon, and other hormones directly into the bloodstream.
The vast majority of pancreatic cancers, over 90%, begin in the exocrine cells lining the pancreatic ducts. These are called pancreatic ductal adenocarcinomas. A smaller proportion arise from the hormone-producing endocrine cells and are called pancreatic neuroendocrine tumours (pNETs). These two types behave very differently and are treated differently.
Types of Pancreatic Cancer
Pancreatic cancer types can be categorised as follows:
- Pancreatic Ductal Adenocarcinoma (PDAC) is by far the most common type. It starts in the cells lining the ducts that carry digestive enzymes out of the pancreas. It is aggressive, tends to spread early, and is the type most people are referring to when they say “pancreatic cancer.” About 70% of PDACs develop in the head of the pancreas, the wider end that sits closest to the small intestine.
- Pancreatic Neuroendocrine Tumours (pNETs) arise from the hormone-producing cells of the pancreas. They are less common and generally grow more slowly than PDAC. Some pNETs are functional, meaning they produce excess hormones and cause specific syndromes, while others are non-functional and discovered incidentally on imaging.
- Acinar Cell Carcinoma is a rare type that starts in the cells producing digestive enzymes. It behaves differently from ductal adenocarcinoma and has a somewhat better prognosis.
- Cystic Tumours of the Pancreas, including intraductal papillary mucinous neoplasms (IPMNs) and mucinous cystic neoplasms, are not always cancerous but carry a risk of malignant transformation. They require careful monitoring and, in some cases, surgery.
Reach Out for Expert Care
Symptoms of Pancreatic Cancer
One of the most difficult aspects of pancreatic cancer is that early disease is almost always silent. Symptoms tend to appear only once the tumour has grown large enough to press on surrounding structures or has begun to spread.
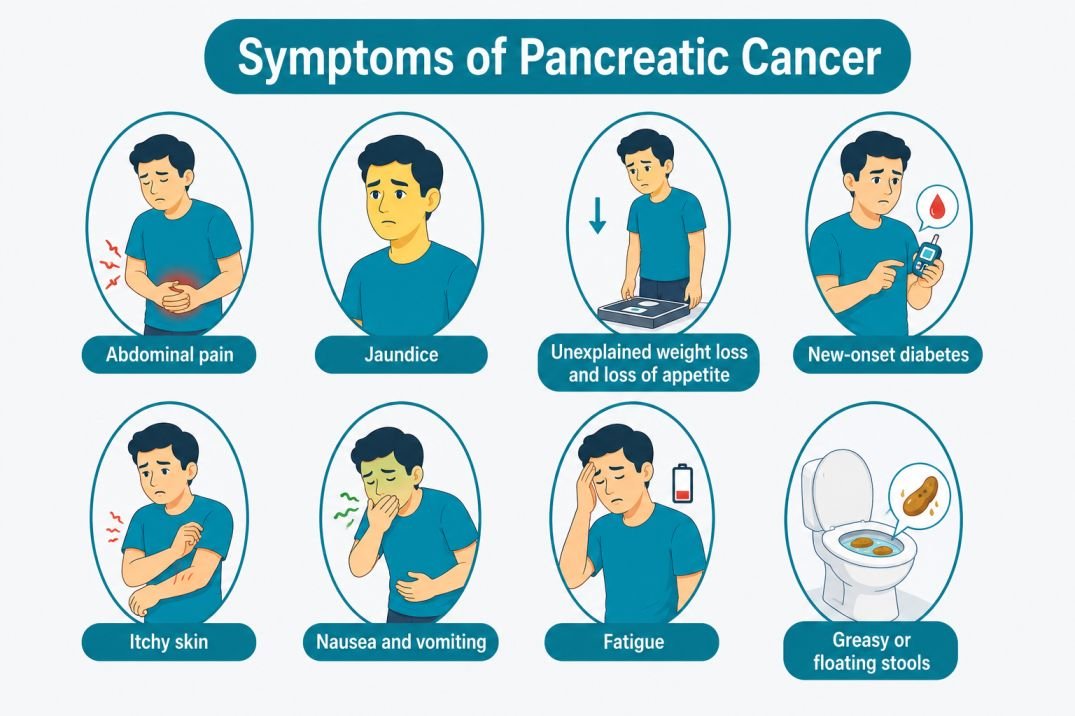
When symptoms do occur, they may include:
- Abdominal pain that radiates to the back, often a dull, persistent ache that is worse when lying down and slightly better when leaning forward
- Jaundice, yellowing of the skin and eyes, dark urine, and pale stools, caused by the tumour blocking the bile duct
- Unexplained weight loss and loss of appetite
- New-onset diabetes in a person with no prior history, or existing diabetes that suddenly becomes harder to control
- Itchy skin, often associated with jaundice
- Nausea and vomiting, particularly if the tumour is pressing on the stomach or duodenum
- Fatigue that is disproportionate to activity level
- Greasy or floating stools caused by poor fat absorption when digestive enzymes are blocked
Jaundice in a middle-aged or older person with no previous liver disease, particularly when it appears alongside weight loss or back pain, should always prompt urgent evaluation. This combination is a recognised warning sign for pancreatic cancer.
Risk Factors for Pancreatic Cancer
Pancreatic cancer does not have a single clear cause, but several factors significantly raise the risk:
- Smoking is the most modifiable risk factor. Smokers are roughly twice as likely to develop pancreatic cancer as non-smokers. The risk decreases after quitting but takes many years to approach that of a non-smoker.
- Diabetes, particularly long-standing Type 2 diabetes, is associated with increased pancreatic cancer risk. Conversely, new-onset diabetes in older adults can sometimes be an early sign of an underlying pancreatic tumour.
- Chronic Pancreatitis, long-term inflammation of the pancreas, often from alcohol use or genetic causes, increases the risk of malignant transformation over time.
- Obesity raises risk, likely through its effects on insulin resistance and inflammation.
- Family History accounts for roughly 10% of pancreatic cancer cases. Having a first-degree relative with pancreatic cancer raises individual risk significantly.
- Genetic Mutations including BRCA2, PALB2, ATM, Lynch syndrome, and familial atypical mole-malignant melanoma (FAMMM) syndrome all increase pancreatic cancer risk. Patients with these mutations may benefit from surveillance programmes.
- Age is a factor, most pancreatic cancers are diagnosed after the age of 60, though it can occur in younger patients, particularly those with hereditary risk.
How Is Pancreatic Cancer Diagnosed?
Because the pancreas is deep inside the abdomen, diagnosing pancreatic cancer requires imaging and tissue testing rather than physical examination alone. Getting the diagnosis right, including the stage, the exact location, and the tumour’s relationship to nearby blood vessels, is critical before any treatment decision is made.
- Ultrasound Abdomen is often the first test ordered when a patient presents with jaundice or abdominal pain. It can detect a pancreatic mass or dilated bile ducts but does not provide the detail needed for surgical planning.
- CT Scan of the Abdomen (Pancreatic Protocol CT) is the most important imaging investigation for pancreatic cancer. A dedicated pancreatic protocol CT uses specific timing and contrast to visualise the tumour, its relationship to the superior mesenteric artery and vein, the portal vein, and other critical structures. It determines whether the tumour is resectable, meaning surgically removable, or not.
- MRI with MRCP (Magnetic Resonance Cholangiopancreatography) provides detailed images of the pancreatic and bile ducts without radiation. It is particularly useful for evaluating cystic lesions and duct involvement.
- Endoscopic Ultrasound (EUS) uses an ultrasound probe attached to an endoscope, which is passed into the stomach. From inside the stomach, it provides very high-resolution images of the pancreas and is the preferred method for obtaining a tissue biopsy from the pancreatic mass. It is accurate, minimally invasive, and does not require a skin incision.
- CT-guided Biopsy, where a needle is inserted through the skin into the pancreatic mass under CT guidance, is used when EUS is not possible or when the tumour is in a location not easily reached by endoscope.
- Blood Tests include liver function tests, a full blood count, and the tumour marker CA19-9. CA19-9 is elevated in many patients with pancreatic cancer and is useful for monitoring treatment response, but it is not a reliable screening test, some patients with pancreatic cancer have normal CA19-9, and it can be elevated in benign conditions like jaundice or pancreatitis.
- PET-CT Scan may be used in selected cases to assess whether the cancer has spread to distant organs before surgery.
Stages of Pancreatic Cancer
Staging determines how far the cancer has spread and is the single most important factor in deciding treatment.
Stage I – The cancer is confined to the pancreas. Stage IA tumours are 2 cm or smaller; Stage IB tumours are between 2 and 4 cm. Surgery is the primary treatment and offers the best chance of cure.
Stage II – The cancer has grown beyond the pancreas but has not yet reached major blood vessels. It may have spread to nearby lymph nodes. Surgery is still possible in many Stage II cases.
Stage III – The cancer has grown into major blood vessels such as the superior mesenteric artery or portal vein, or has spread more extensively to lymph nodes. Some Stage III tumours are considered borderline resectable, not immediately operable but potentially operable after chemotherapy shrinks the tumour. Others are locally advanced and not operable at the time of diagnosis.
Stage IV – The cancer has spread to distant organs, most commonly the liver, lungs, or peritoneum. Surgery is not typically performed for Stage IV pancreatic cancer, and treatment focuses on systemic therapy and quality of life.
It is worth noting that a significant proportion of patients initially classified as borderline resectable or locally advanced can be converted to resectable status after a course of chemotherapy, a strategy called neoadjuvant chemotherapy. This is why evaluation at a specialist centre with experienced surgeons is important even when the cancer initially appears inoperable.
Treatment Options for Pancreatic Cancer
Surgery
Surgery is the only treatment that offers a genuine chance of cure for pancreatic cancer. Only patients with localised disease, Stage I, II, and selected Stage III, are candidates for surgery. Despite this, surgery should always be considered and evaluated at a specialist centre, because the assessment of resectability requires both expert imaging review and surgical experience.
- Whipple’s Procedure (Pancreaticoduodenectomy) is the most commonly performed operation for pancreatic cancer. It is used for tumours in the head of the pancreas, which is where most PDACs develop. The operation removes the head of the pancreas, the duodenum (first part of the small intestine), the gallbladder, the lower part of the bile duct, and nearby lymph nodes. The remaining pancreas, bile duct, and stomach are then reconnected to the intestine to restore the digestive pathway.
The Whipple procedure is one of the most complex operations in abdominal surgery. It requires a surgeon with significant experience in pancreatic surgery, both for the resection itself and for managing the reconstruction and potential complications. Outcomes are directly linked to surgeon and centre volume.
- Distal Pancreatectomy removes the body and tail of the pancreas, the left side of the gland, and is used for tumours in this region. The spleen is often removed at the same time.
- Total Pancreatectomy removes the entire pancreas and is performed when the tumour involves the whole gland or when the pancreatic tissue quality makes reconstruction after a Whipple or distal procedure unsafe. Patients who have the entire pancreas removed will need lifelong insulin injections and pancreatic enzyme supplements, but can live well with these.
- Vascular Resection and Reconstruction is performed at highly specialised centres when the tumour involves major blood vessels like the portal vein or superior mesenteric vein. The affected segment of the vessel is removed and reconstructed using a graft. This extends the option of curative surgery to patients who would otherwise be considered inoperable.
Robotic Pancreatic Surgery
Robotic surgery has changed what is possible in complex pancreatic operations. The robotic platform provides a magnified, three-dimensional view inside the abdomen and allows the surgeon to work with precision in a small, confined space, advantages that matter greatly when operating near major blood vessels and delicate pancreatic tissue.
Robotic Whipple procedures and robotic distal pancreatectomies, in experienced hands, offer patients the same oncological outcomes as open surgery, with the benefits of smaller incisions, less blood loss, reduced postoperative pain, shorter hospital stay, and faster return to normal activity.
Dr. Surender Kumar Dabas is among the very few surgical oncologists in Delhi performing robotic pancreatic surgery. As one of the best robotic cancer surgeons in India, with over 5,000 robotic procedures performed, he offers robotic pancreatic surgery at Manipal Comprehensive Cancer Centre, one of the few centres in North India to provide this level of care. Patients from Rohtak, Kanpur, and across Delhi NCR seek him for pancreatic cancer surgery in Delhi, including complex cases involving vascular involvement.
Chemotherapy
Chemotherapy is used across all stages of pancreatic cancer, in different ways depending on the clinical situation.
- Neoadjuvant Chemotherapy is given before surgery to shrink borderline resectable or locally advanced tumours, with the aim of making them operable. Regimens commonly used include FOLFIRINOX (a combination of four drugs) and gemcitabine plus nab-paclitaxel.
- Adjuvant Chemotherapy is given after surgery to reduce the risk of the cancer returning. Modified FOLFIRINOX is currently the preferred regimen for patients who are fit enough to tolerate it.
- Palliative Chemotherapy is used in Stage IV disease to slow tumour growth, control symptoms, and prolong survival. It does not cure cancer but can meaningfully extend good-quality life in many patients.
Radiation Therapy
Radiation is not used routinely in pancreatic cancer but plays a role in specific situations. Chemoradiation, combining chemotherapy with radiation, is used for locally advanced tumours that cannot be surgically removed. It may also be given after surgery in selected cases to reduce the risk of local recurrence. Stereotactic Body Radiotherapy (SBRT) is a newer technique that delivers high, precisely focused doses to the tumour over a small number of sessions and is being increasingly used in locally advanced pancreatic cancer.
Targeted Therapy
A small subset of pancreatic cancers carry genetic mutations that can be targeted with specific drugs. Olaparib, a PARP inhibitor, is approved for patients with BRCA1 or BRCA2 mutations whose cancer has not progressed after platinum-based chemotherapy. Entrectinib and larotrectinib are used for the rare NTRK fusion-positive pancreatic cancers. Molecular profiling of the tumour, testing for these mutations, is now recommended for all patients with metastatic pancreatic cancer.
Palliative and Supportive Care
For patients with advanced pancreatic cancer where curative treatment is not possible, a dedicated palliative care team works alongside the oncology team to manage symptoms, maintain quality of life, and support both the patient and their family. This includes pain management, nutritional support, management of jaundice (through biliary stenting), and psychological support. Palliative care is not about giving up, it is about making sure that the time patients have is as comfortable and meaningful as possible.
Cost of Pancreatic Cancer Surgery in Delhi NCR
The cost of pancreatic cancer surgery in Delhi NCR is between ₹3,50,000 and ₹18,00,000 depending on the type of procedure, robotic or open, the complexity of the case, and the hospital. For a personalised cost estimate based on your specific diagnosis, contact Dr. Dabas’s clinic directly for a consultation.
Life After Pancreatic Cancer Treatment
Recovery after major pancreatic surgery is gradual. The Whipple procedure is a complex operation and patients should expect a hospital stay of 7–10 days, with full recovery taking 6–8 weeks. Robotic approaches generally allow faster recovery than open surgery.
Long-term follow-up after treatment includes:
- CT scans every 3–6 months for the first two years, then annually
- CA19-9 blood tests at each follow-up visit
- Monitoring for diabetes and pancreatic enzyme insufficiency
- Nutritional support and dietary adjustments, particularly after total pancreatectomy
- Adjuvant chemotherapy coordination where applicable
Most patients who have had part of the pancreas removed will need pancreatic enzyme replacement therapy (PERT), tablets taken with every meal to help digest food. Those who develop diabetes after surgery will need insulin management. Both of these are manageable conditions that most patients adapt to well over time.
Why Choose a Specialist for Pancreatic Cancer Surgery?
Pancreatic cancer surgery, particularly the Whipple procedure, is among the most technically demanding operations in all of surgery. Studies consistently show that outcomes are significantly better at high-volume centres with experienced surgeons: lower complication rates, fewer leaks, shorter hospital stays, and better long-term survival.
This is not a surgery to have done at the nearest available hospital. It requires a surgeon who does these regularly, a team experienced in managing pancreatic surgery complications, and a centre equipped to handle complex reconstructions, including vascular involvement.
Dr. Surender Kumar Dabas is a best surgical oncologist in India with focused expertise in hepatopancreatic and biliary cancers. Operating at Manipal Comprehensive Cancer Centre, he brings over 30,000 cancer surgeries and 5,000+ robotic procedures to each case. Patients from Gurgaon searching for the best pancreatic cancer doctor in Gurgaon, patients from Kanpur looking for a pancreatic cancer doctor in Kanpur, and patients from across Delhi NCR come to him for surgical evaluation, including second opinions on cases deemed inoperable elsewhere.
Conclusion
Pancreatic cancer is a serious diagnosis, but the picture is not as bleak as it once was. Surgery, when it is possible, offers real hope. Chemotherapy regimens are more effective than they were a decade ago. And robotic surgery has made complex pancreatic operations safer and more accessible for the right patients. What has not changed is this: outcomes are directly tied to where you are treated and who treats you. Whether you are looking for the best pancreatic cancer doctor in Rohtak, a surgical oncologist in Delhi for a second opinion, or a specialist experienced in robotic cancer surgery in Delhi NCR for a complex case, early expert evaluation is the most important step you can take. Dr. Surender Kumar Dabas sees patients from across North India, from straightforward resectable cases to the most complex, multi-vessel disease. If you or someone in your family has been diagnosed with pancreatic cancer, do not delay getting a specialist opinion. The window for surgical intervention, where it exists, is time-sensitive.

Dr. Surender Dabas' Medical Content Team
Dr. Surender Dabas' Medical Content Team is committed to providing accurate, reliable, and easy-to-understand information on cancer care. Working closely with oncology experts, the team ensures that every article is medically reviewed, up-to-date, and designed to help patients and their families better understand cancer, treatment options, and recovery.
