Prostate Cancer Treatment in Delhi NCR
Prostate cancer is one of the most common cancers in men globally and cases are rising steadily across Delhi, Gurgaon, and the wider NCR region. The good news is that when caught early and treated by the right specialist, prostate cancer is one of the most manageable cancers a man can face.
Patients from Gurgaon, Delhi, Faridabad, and across North India consult Dr. Surender Kumar Dabas, one of the best robotic cancer surgeons in India, for Prostate Cancer Treatment in Delhi NCR, robotic radical prostatectomy, and comprehensive urological cancer care at Manipal Comprehensive Cancer Centre.
What Is Prostate Cancer?
The prostate is a small, walnut-shaped gland located deep in the male pelvis, just below the bladder and in front of the rectum. It produces seminal fluid that nourishes and transports sperm. Because the prostate surrounds the urethra, the tube through which urine and semen leave the body, prostate problems often first appear as urinary symptoms.
Prostate cancer develops when cells in the prostate gland begin to grow abnormally and divide out of control. It is not one disease. Some prostate cancers are slow-growing, may never cause symptoms, and require only careful monitoring. Others are aggressive, spread quickly, and need prompt treatment. Accurate diagnosis, proper staging, and matching the right treatment to the right patient is why specialist evaluation matters.
Benign vs. Malignant Prostate Disease
Not all prostate growths are cancer, and understanding the difference helps patients make better decisions.
Benign Prostatic Hyperplasia (BPH) is a non-cancerous enlargement of the prostate, extremely common in men over 50. It causes urinary symptoms such as frequent urination, weak flow, and difficulty starting, but it does not spread and is not life-threatening. BPH and prostate cancer can coexist, and having BPH does not increase cancer risk.
Prostate Cancer is a malignant growth that can invade surrounding structures, spread to pelvic lymph nodes, and metastasise to distant organs, most commonly the bones. The distinction between BPH and prostate cancer cannot be made on symptoms alone. PSA testing and, where indicated, biopsy are required.
Reach Out for Expert Care
Types of Prostate Cancer
- Adenocarcinoma accounts for over 95 percent of prostate cancers. It arises from the glandular cells that produce seminal fluid. When most people and doctors refer to prostate cancer, this is what they mean.
- Small Cell Carcinoma of the prostate is rare but aggressive. It does not produce PSA and does not respond to hormone therapy. It is treated similarly to small cell lung cancer.
- Ductal Adenocarcinoma arises in the ducts of the prostate and tends to be more aggressive than standard adenocarcinoma.
- Neuroendocrine Tumours of the prostate are rare and can develop on their own or as a transformation of previously treated adenocarcinoma.
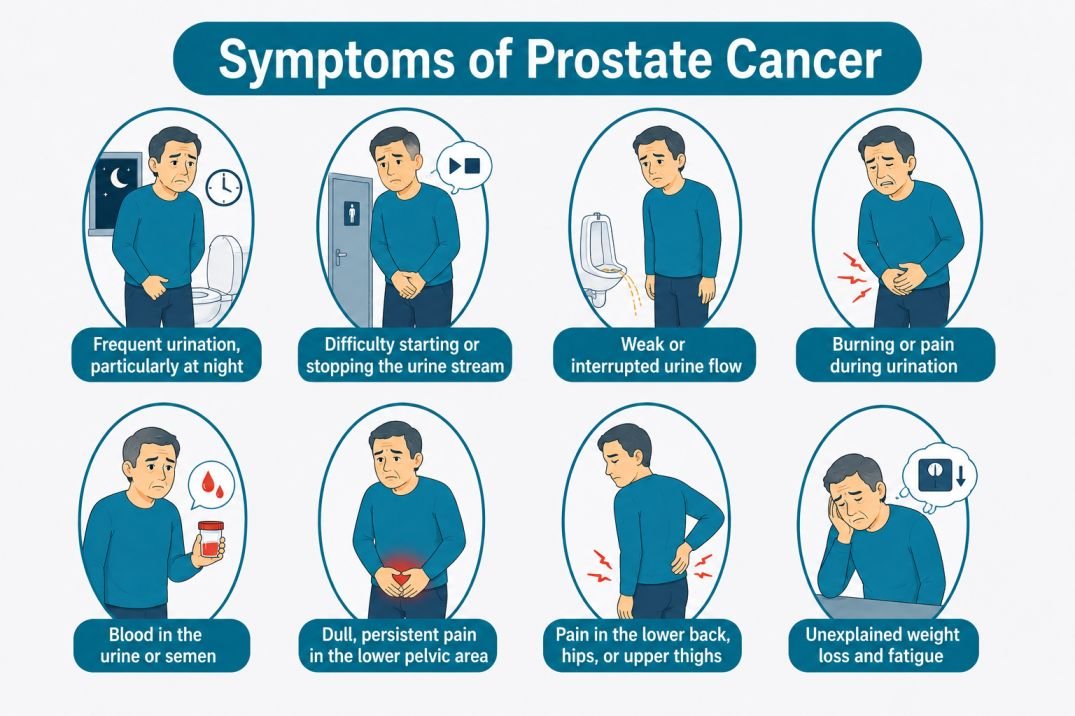
Symptoms of Prostate Cancer
Early prostate cancer often produces no symptoms at all. By the time symptoms appear, the cancer has usually progressed beyond the earliest, most treatable stage. This is why PSA screening in high-risk and older men is so important.
When symptoms do occur, they may include:
- Frequent urination, particularly at night
- Difficulty starting or stopping the urine stream
- Weak or interrupted urine flow
- Burning or pain during urination
- Blood in the urine or semen
- Dull, persistent pain in the lower pelvic area
- Pain in the lower back, hips, or upper thighs, which may suggest spread to bone
- Unexplained weight loss and fatigue in advanced disease
Many of these symptoms overlap with BPH. Urinary symptoms alone do not mean cancer, but they do mean a man should be evaluated, particularly if he is over 50 or has risk factors for prostate cancer.
Risk Factors for Prostate Cancer
- Age is the single strongest risk factor. Prostate cancer is rare under 40. Risk increases sharply after 50 and the majority of cases are diagnosed in men over 65.
- Family History significantly raises risk. Having a father or brother with prostate cancer more than doubles a man’s risk, particularly if the relative was diagnosed at a younger age.
- Genetic Mutations, particularly in BRCA1, BRCA2, and Lynch syndrome-associated genes, raise prostate cancer risk. Men with BRCA2 mutations are at particular risk of aggressive disease. Genetic testing is recommended for men with a strong family history.
- Race and Ethnicity play a role. Prostate cancer is more common in men of African descent, who also tend to be diagnosed younger and with more aggressive disease.
- Diet high in red meat, processed foods, and dairy has been associated with modestly increased risk. A diet rich in vegetables, particularly tomato-based foods, may be protective.
- Obesity is linked to a higher risk of aggressive prostate cancer and greater risk of dying from the disease.
Screening for Prostate Cancer
Prostate cancer screening uses two tools together:
PSA Blood Test measures Prostate-Specific Antigen, a protein produced by both normal and cancerous prostate cells. A PSA level above 4 ng/mL is generally the threshold for further investigation, though some doctors use lower cut-offs of 2.5 to 3 ng/mL in younger men or those with risk factors. A high PSA alone does not confirm cancer; it can be elevated by BPH, prostatitis, and other benign conditions. PSA levels between 4 and 10 ng/mL carry roughly a 25 percent chance of cancer. Above 10 ng/mL, the probability rises above 50 percent.
Digital Rectal Examination (DRE) allows the doctor to feel the prostate for hard, nodular, or irregular areas that may suggest cancer. DRE is used alongside PSA and can detect cancers that do not significantly raise PSA.
Screening is recommended annually from age 50 for average-risk men, and from age 40 to 45 for men with a family history of prostate cancer or known BRCA2 mutations.
How Is Prostate Cancer Diagnosed?
A raised PSA or abnormal DRE raises suspicion but does not confirm cancer. Diagnosis requires a biopsy.
- Multiparametric MRI (mpMRI) of the Prostate is now performed before biopsy in most cases. It identifies suspicious areas and grades them using the PI-RADS scoring system (1 to 5). Higher scores indicate higher probability of significant cancer. MRI-guided biopsy dramatically improves detection of clinically significant cancer while reducing unnecessary procedures.
- Transrectal Ultrasound-Guided (TRUS) Biopsy uses ultrasound to guide a thin needle through the rectal wall into the prostate to collect tissue samples, typically 12 core samples from different regions.
- Fusion Biopsy (MRI-Ultrasound Fusion) overlays MRI images onto real-time ultrasound during the biopsy, allowing targeted sampling of specific suspicious areas identified on MRI, improving accuracy compared to systematic biopsy alone.
- Transperineal Biopsy accesses the prostate through the skin between the scrotum and anus rather than through the rectum. It is increasingly preferred as it carries a lower risk of infection.
Understanding the Pathology Report: Gleason Score and Grade Groups
Once the biopsy is analysed, the pathologist assigns a grade based on how abnormal the cells look under the microscope. This grading is critical as it indicates how aggressive the cancer is likely to be.
Gleason Score identifies the two most dominant cancer patterns in the tissue and assigns each a grade from 1 to 5. These are added together. A Gleason score of 6 (3+3) represents the lowest grade seen in practice; a score of 10 (5+5) represents the most aggressive.
Grade Groups map directly to Gleason scores and provide clearer prognostic information:
- Grade Group 1 (Gleason 6): Low-grade. Slow-growing. Active surveillance often appropriate.
- Grade Group 2 (Gleason 3+4=7): Intermediate-grade. Treatment usually recommended.
- Grade Group 3 (Gleason 4+3=7): Intermediate-high grade. Treatment strongly recommended.
- Grade Group 4 (Gleason 8): High-grade. Prompt treatment required.
- Grade Group 5 (Gleason 9 to 10): Highest grade. Aggressive disease requiring urgent treatment.
The distinction between 3+4 and 4+3 matters. Men with 4+3=7 have meaningfully worse outcomes than those with 3+4=7, even though both add up to 7.
Staging of Prostate Cancer
Stage I – Cancer is confined to a small area of the prostate. Grade Group 1. Very low risk. Active surveillance is often preferred.
Stage II – Cancer is confined to the prostate but is larger, more detectable, or higher grade. Surgery or radiation is recommended for most Stage II cases.
Stage III – Cancer has grown beyond the prostate, involving the seminal vesicles or nearby structures. Treatment involves surgery, radiation with hormone therapy, or a combination.
Stage IV – Stage IVA means cancer has spread to pelvic lymph nodes. Stage IVB means it has spread to distant organs, most commonly bone. Stage IV is primarily managed with systemic therapy, though selected patients may still benefit from surgery or radiation.
Prostate Cancer Treatment Options in Delhi NCR
Prostate Cancer Treatment depends on the stage, grade, PSA level, and the patient’s overall health and personal priorities. Modern treatment may involve surgery, radiation therapy, hormone therapy, targeted therapy, immunotherapy, or a carefully planned combination.
-
Active Surveillance
For low-risk, slow-growing prostate cancers, particularly Grade Group 1, active surveillance is a medically sound option. This means monitoring the cancer closely with regular PSA tests, DRE, repeat MRI, and periodic biopsies rather than treating immediately. The goal is to avoid the side effects of treatment in men whose cancer is unlikely to progress, while intervening promptly if the disease changes.
Active surveillance is not ignoring the cancer. It is a structured, evidence-based approach that avoids over-treating cancers that may never cause harm.
-
Surgery: Radical Prostatectomy
Radical prostatectomy, the surgical removal of the entire prostate gland, seminal vesicles, and pelvic lymph nodes, is one of the two primary curative treatments for localised prostate cancer alongside radiation therapy.
The goals of surgery are complete cancer removal with clear margins, preservation of urinary continence, and, where oncologically safe, preservation of the nerve bundles responsible for erectile function (nerve-sparing prostatectomy).
-
Robotic Radical Prostatectomy
Robotic Radical Prostatectomy has become the gold standard for surgical treatment of prostate cancer at high-volume specialist centres. The prostate sits deep in the pelvis, surrounded by the bladder, rectum, urethra, and the delicate neurovascular bundles controlling erection and continence. Operating in this confined space with the precision required to remove cancer completely while protecting these structures is where the robotic platform excels.
The robotic system provides a magnified, three-dimensional view deep inside the pelvis and allows the surgeon to work with finely controlled instrument movements that are not possible in open or standard laparoscopic surgery. For patients, this translates into significantly less blood loss, shorter hospital stay, faster return to urinary control, and better preservation of sexual function compared to open surgery.
Dr. Surender Kumar Dabas is one of the best robotic cancer surgeons in India and a leading prostate cancer specialist in Gurgaon and Delhi NCR. As a best surgical oncologist in India with over 5,000 robotic cancer surgeries performed, he offers Robotic Radical Prostatectomy at Manipal Comprehensive Cancer Centre, bringing a level of surgical experience and precision that very few surgical oncologists in Delhi can match. Men from Gurgaon, Delhi, Faridabad, and across North India seek Dr. Dabas for prostate cancer treatment in Gurgaon and robotic cancer surgery in Delhi NCR.
-
Radiation Therapy
Radiation therapy is an equally effective curative option for localised and locally advanced prostate cancer, preferred in certain situations, particularly for older patients, those with significant other health conditions, or those with locally advanced disease.
External Beam Radiation Therapy (EBRT) using modern techniques like IMRT and IGRT delivers precisely targeted radiation to the prostate while minimising dose to the bladder and rectum.
Stereotactic Body Radiotherapy (SBRT) delivers high-dose, precisely focused radiation over just 5 sessions, increasingly used for low- and intermediate-risk localised prostate cancer.
- Brachytherapy involves placing radioactive seeds or a temporary radioactive source directly inside the prostate and is used for selected low- and intermediate-risk cases.
-
Hormone Therapy (Androgen Deprivation Therapy)
Prostate cancer cells depend on testosterone to grow. Hormone therapy reduces testosterone levels, depriving the cancer of the signal it needs to proliferate. It is used alongside radiation for intermediate and high-risk disease, as the primary treatment for advanced or metastatic prostate cancer, and to control recurrence after initial treatment.
Hormone therapy does not cure prostate cancer but can control it for months to years in many patients. It is given as injections (LHRH agonists or antagonists) or oral drugs including enzalutamide, abiraterone, and darolutamide.
-
Chemotherapy
Chemotherapy is used in metastatic prostate cancer that is newly diagnosed with high-volume disease or has become resistant to hormone therapy (castration-resistant prostate cancer). Docetaxel is the standard first-line chemotherapy agent; cabazitaxel is used after docetaxel failure.
-
Targeted Therapy
Men with BRCA1, BRCA2, or other DNA repair gene mutations whose prostate cancer has spread and progressed on hormone therapy may benefit from PARP inhibitors, specifically olaparib and rucaparib. Genetic testing is now recommended for all men with metastatic prostate cancer.
-
Immunotherapy
Pembrolizumab is approved for prostate cancers with microsatellite instability or mismatch repair deficiency. Immunotherapy has a more limited role in prostate cancer than in some other tumour types, but ongoing clinical trials are expanding its application.
-
Bone-Directed Therapy
Because prostate cancer frequently spreads to bone, managing bone metastases is an important component of care for advanced disease. Radium-223 targets bone metastases and has been shown to extend survival in castration-resistant prostate cancer. Bone-strengthening agents like zoledronic acid and denosumab reduce the risk of fractures and bone pain.
Cost of Prostate Cancer Treatment in Delhi NCR
The cost of Prostate Cancer Treatment in Delhi NCR is between ₹1,50,000 to ₹25,00,000 depending on the treatment approach, whether robotic surgery, radiation, hormone therapy, or a combination, and the complexity of the case. For a personalised cost estimate based on your diagnosis and stage, contact Dr. Surender Dabas‘s team directly at 8796173403.
Life After Prostate Cancer Treatment
Recovery after Robotic Radical Prostatectomy is significantly faster than after open surgery. Most patients are discharged within one to two days and return to light activity within two to three weeks. A urinary catheter is typically in place for seven to ten days after surgery.
- Urinary control returns in the majority of patients, though it takes time, weeks to months depending on the individual. Pelvic floor exercises started before and after surgery speed recovery.
- Erectile function recovery depends on whether nerve-sparing surgery was performed and the patient’s baseline function before surgery. In nerve-sparing cases performed by an experienced robotic cancer surgeon, meaningful recovery is possible in a significant proportion of men.
Long-term follow-up includes:
- PSA testing every 3 to 6 months for the first two years, then annually
- A PSA that remains undetectable after surgery is the best indicator of successful cancer removal
- Any PSA rise after treatment, called biochemical recurrence, requires prompt evaluation
Why Surgeon and Centre Selection Matters in Prostate Cancer?
Robotic Radical Prostatectomy is among the most technically demanding urological operations. The proximity of the bladder, rectum, urethra, and neurovascular bundles to the prostate means that outcomes, both cancer control and functional recovery, are directly linked to surgical volume and experience.
Studies consistently show that high-volume robotic surgeons achieve better cancer-free margins, better continence recovery, and better preservation of sexual function than lower-volume counterparts.
Dr. Surender Kumar Dabas is a best surgical oncologist in India with a specific focus on urological and robotic cancer surgery. He is recognised as the best doctor for prostate surgery in Gurgaon, a leading urological cancer specialist in Gurgaon, and one of the best robotic surgeons in Delhi NCR, with over 5,000 robotic procedures performed at Manipal Comprehensive Cancer Centre. Patients from Gurgaon, Faridabad, Delhi, and across North India seek him for prostate cancer treatment in Gurgaon and robotic cancer surgery in Delhi NCR, from straightforward localised disease to complex, high-risk cases requiring nerve-sparing surgery or extended lymph node dissection.
Conclusion
Prostate cancer is common, but when caught early and treated by the right specialist, it is also one of the most manageable cancers a man can face. The range of treatment options available today, from active surveillance for low-risk disease through to Robotic Radical Prostatectomy, radiation, and advanced systemic therapies for metastatic disease, means that almost every patient has a meaningful path forward.
What matters most is getting an accurate diagnosis, proper staging, and specialist-level evaluation before any treatment decision is made. Whether you are looking for the best doctor for prostate surgery in Gurgaon, a surgical oncologist in Delhi for a second opinion, or a specialist in robotic cancer surgery in Delhi NCR, Dr. Surender Kumar Dabas at Manipal Comprehensive Cancer Centre sees patients from across North India, from straightforward early-stage cases to the most complex, high-risk disease.
If you have been diagnosed with prostate cancer, or your PSA has come back elevated, do not delay getting a specialist opinion. Early evaluation changes outcomes.

Dr. Surender Dabas' Medical Content Team
Dr. Surender Dabas' Medical Content Team is committed to providing accurate, reliable, and easy-to-understand information on cancer care. Working closely with oncology experts, the team ensures that every article is medically reviewed, up-to-date, and designed to help patients and their families better understand cancer, treatment options, and recovery.
